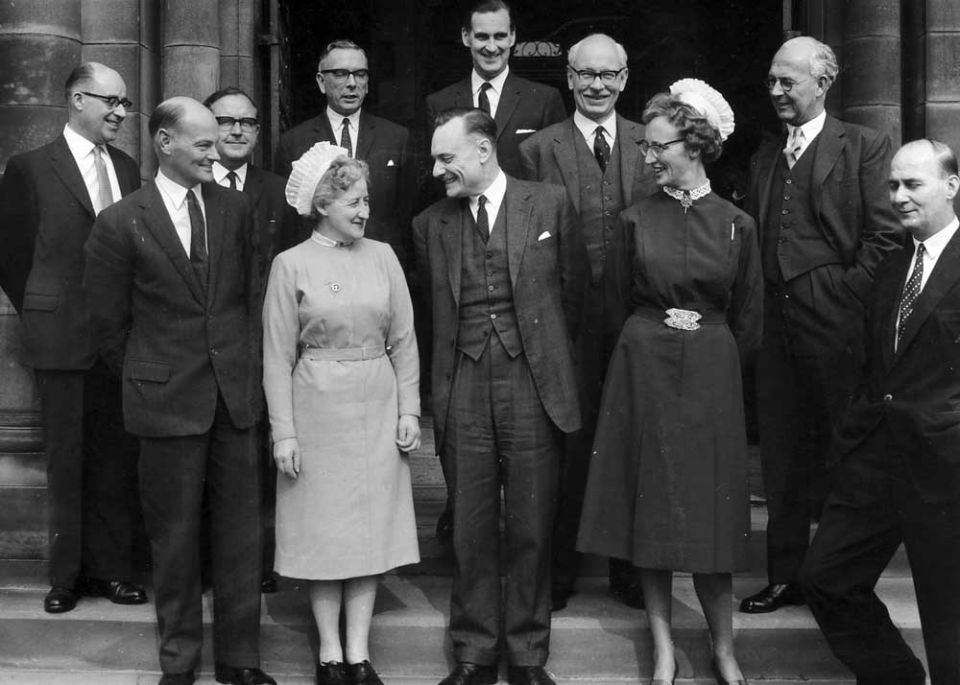














| Enoch Powell, Brighton in 1961 at the National Association for Mental Health (now Mind) annual conference. It was there that then health minister Enoch Powell signaled the end of the old asylums with his historic “water-tower” speech. He described the institutions thus: “There they stand, isolated, majestic, imperious, brooded over by the gigantic water-tower and chimney combined, rising unmistakable and daunting out of the countryside.” The Rt. Hon. J. Enoch Powell Minister of Health It was a year ago that my predecessor, Derek Walker-Smith, came here to open your last Conference which, as your Chairman has reminded you, was the first one to be held after the passage into law – though not yet after the coming into effect – of the Mental Health Act, in which he himself had taken an important part. This year I am no less glad than he was to be with you at your opening session – it is not the only thing to which I succeeded him as Minister of Health since the inception in January of this year of long term planning in the hospital service.The theme of your Conference this year is an integrated service for mental disorders, and this could not possibly chime more perfectly with the aspirations to which the long term planning for our hospital service is intended to give expression. So important is that planning operation on which you are now engaged, that I am afraid I tend to relate to it, in some way or another, almost everything in the whole field of health far and near.I am afraid il has become a preoccupation with me, almost an obsession, and I hope you will bear with me, therefore, if for a few minutes I talk about the relationship between this 10-year hospital plan and that concerned with the future of mental health, which has brought us all together this morning.The essential idea of the plan is to get on to paper a picture or, statement of the pattern of hospital provision which we think right and practicable for this country in the mid 1970s. From that statement and a comparison of it with what is “on the ground” today there must emerge logically a programme showing the work which needs to be completed or commenced – and also the premises and provisions which need to be eliminated – during the course of the present decade. But that statement itself, that picture of the hospital pattern of the mid 1970s – 15 years ahead – must rest in turn upon a foundation, and an assessment of the then demand for hospital care of various kinds. Such an assessment is nothing less than a forecast and expression of intention which embraces the future of all branches of the National Health Service, indeed of every aspect of the nation’s provision for health.
However tentative, however qualified, however much in need of the revision which it will receive in each succeeding year, this plan must thus embody our aims and ambitions, our vision of the future for 15 years ahead. Let me apply this now to mental health, a field in which the advances in psychiatric knowledge and methods offer a standing challenge to the National Health Service to provide the setting in which that knowledge and those methods can yield their fullest benefit. I have intimated to the hospital authorities who will be producing the constituent elements of the national hospital plan that in 15 years time there may well be needed not more than half as many places in hospitals for mental illness as there are today. Expressed in numerical terms, this would represent a redundancy of no fewer than 75,000 hospital beds. Even so, I would say that if we err, we would rather err on the side of under-estimating the provision which ought to be required in hospitals 15 years from now. This 50 per cent reduction itself is only a statistical projection by the General Register Office of the fall in demand based upon present trends. Yet there is not a person present whose ambition is not to speed up those present trends. So if we are to have the courage of our ambitions, we ought to pitch the estimate lower still, as low as we dare, perhaps lower. But that 50 per cent or less of present places in hospitals for the mentally sick – what will they look like and where will they be ? We know already what ought to be the answer to that question: they ought for the most part to be in wards and wings of general hospitals. Few ought to be in great isolated institutions or clumps of institutions, though I neither forget nor underestimate the continuing requirements of security for a small minority of patients. Now look and see what are the implications of these bold words. They imply nothing less than the elimination of by far the greater part of this country’s mental hospitals as they exist today. This is a colossal undertaking, not so much in the new physical provision which it involves, as in the sheer inertia of mind and matter which it requires to he overcome. There they stand, isolated, majestic, imperious, brooded over by the gigantic water-tower and chimney combined, rising unmistakable and daunting out of the countryside – the asylums which our forefathers built with such immense solidity to express the notions of their day. Do not for a moment underestimate their powers of resistance to our assault. Let me describe some of the defences which we have to storm. First there is the actual physical solidity of the buildings themselves: the very idea of these monuments derelict or demolished arouses an instinctive resistance in the mind. At least, we find ourselves thinking,
Well, let me here declare that if we err, it is our duly to err on the side of ruthlessness. For the great majority of these establishments there is no appropriate future use, and I for my own part will resist any attempt to foist another purpose upon them unless it can be proved to me in each case that, such, or almost such, a building would have had to be erected in that, or some similar, place to serve the other purpose, if the mental hospital had never existed. “Not Building Pyramids” We have to .strive to alter our whole mentality about hospitals, and about mental hospitals especially. Hospital building is not like pyramid building, the erection of memorials to endure to a remote posterity. We have to get the idea into our heads that a hospital is a shell, a framework, however complex, to contain certain processes, and when the processes change or are superseded, then the shell must most probably be scrapped and the framework dismantled. The old Roman virtue of pie tax becomes a vice when it is directed towards a hospital building. Then again much of what we have done in the last decade to improve these mental hospitals has made the right course from now on more difficult still. We have spent money–and who shall blame us if we have used the resources to our hand in making conditions less inadequate for the present generation of chronic mental patients while it remains ? – on “up-grading” the old wards, building annexes and villas, improving here, modifying there; and then is someone going to come along and put a “life” upon our handiwork. and say to us “All this must be swept away anyhow” ? There comes a point where the very improvement of existing facilities militates powerfully against their supersession by something different and better. The resistance is not only physical. Hundreds of men and women, professional or voluntary, have given years, even lifetimes, to the service of a mental hospital or a group of mental hospitals. They have laboured devotedly, through years of scarcity and neglect, to render the conditions in them more tolerable, and of late they have seized with delight upon the new possibilities opening up, and the new resources available, for these old but somehow cherished institutions. From such bodies it demands no mean moral effort to recognise that the institutions themselves are doomed. It would be more than flesh and blood to expect them to take the initiative in planning their own abolition, to be the first to set the torch to the funeral pyre. Finally, the transformation of the mental hospitals is not only a matter of buildings, the change of a physical pattern, it is also the transformation of a whole branch of the profession of medicine, of nursing, of hospital administration. Politics apart, let us admit that we all have a great deal of the conservative in our make-up, and find it easier to envisage things going on much as at present, or with small or gradual modifications, than deliberately to choose and favour the unaccustomed, the drastic and voluntarily to bring about a pattern of organisation in which new tasks will be performed in a new and wider setting. With all these built-in tendencies to perpetuate the old, I am certain of this, that it is the duty of a Minister of Health and the duty of the National Association for Mental Health, to lean with all their might in the opposite direction: to choose and to favour wherever they have the choice, the course of more drastic and fundamental change: for we may be pretty sure that even so the progress of medical thought and method will still be well on ahead of our practice. So far I have been talking mainly of the hospitals for the mentally ill, and I have been looking at the hospital side of the equation. When we look at the future of provision for the sub- normal, the prospects for change must seem far less dramatic – certainly if we discount, as I suppose we prudently ought, the chance of some medical “break through” on this front. Far from contemplating the certainty of a heavy run-down in numbers, we have here to reckon with the increase which flows automatically from the lengthened expectation of life of the sub-normal and their improved prospects of surviving infancy. This does not mean, however, that we ought passively to accept a corresponding increase in hospital places or the perpetuation of the present hospital pattern. I have the impression that we know much less than we ought about the prevalence, variety and management of subnormality, but handicapped though we may be at present by these deficiencies, the hospital plan has here also to be founded upon an assessment of need which leans as far as possible in the direction of the trends that we want to favour. This brings me of course to the complement of the hospital pattern, the pattern of provision in the community. It would be quite unrealistic to attempt to state what is intended, and what is not intended, by way of hospital provision in the 1970s and not to spell out with as much precision and detail as is practicable all thai this implies in terms of care outside the hospitals. I will go so far as to say that a hospital plan makes no sense unless the medical profession outside the hospital service will be able progressively to accept responsibility for more and more of that care of patients which today is given inside the hospitals. It makes no sense therefore unless the medical profession outside the hospital service can be supported in this task by a whole new development of the local authority services for the old, for the sick and for the mentally ill and mentally subnormal. That is why, at the earliest moment possible, I intend to call on local health and welfare authorities, through the bodies which represent them, to take a hand in mapping the joint future of the hospital and the local authority services. There are two aspects to the development of the local authority services, the human and the physical – the recruitment and training of the necessary staff of the right kind and quality, and the provision of the range of different types of building which will be required, I stress this characteristic of variety, because one of the important qualities of local authority provision outside the hospital service is the precision with which it ought to be able to cater for a whole gamut or gradation of different degrees of need. The transition between hospital and the outside world, for all that we can ever do to narrow or bridge the gap, will always necessarily be an abrupt one. On the other hand, if armed with the necessary capital provision, the local authorities can achieve an almost unlimited range of gradation between the complete independence of full mental and physical health and the almost complete dependence of the old or subnormal whose need for care and attention is little short of that which only a hospital can provide. Indispensable, however, though the appropriate physical equipment is, I doubt if now the availability of finance is the factor which limits its provision. The capital expenditure of local health and welfare authorities this year has been fully half as large as the capital expenditure on the hospital service itself, and I expect that something like that ratio will be maintained – with, of course, increasing absolute figures – for a number of years to come. What I believe is urgent is a much clearer and more definite statement than we yet possess, of the need, and of the provision for it, at which local authorities are aiming. In fact, the community counterpart of the long-term hospital plan ought to be as effective a formative and driving influence outside the hospital service as the hospital plan itself is inside. Its influence should also be felt upon the other element in the local authority services, the human factor. In the last resort, it is the consciousness of a great and expanding task to be performed, of a great service which is destined to develop in the coming decades, which alone will secure the flow of personnel into community care. Here also is a region as yet but partially mapped. In this year, 1961 we intend to erect the initial scaffolding of a professional training for the social worker, and to link that with the training of other elements in the staff of the community services. But it is the pull exerted by an evident demand and a conscious purpose which, alone, will ensure that the training courses are filled and that the establishments are staffed. It might seem to you that although I am nearing the end of what I have to say, I have so far scarcely referred at all to yourselves – to that Annual Conference which I am opening. In reality, every word of what I have said has been directed towards you: and that phrase “conscious purpose” is the key. None of these ambitions that I have been describing can be fulfilled, none of these changes, drastic and difficult, in the pattern of our provision for the mentally ill and afflicted can be brought about, unless the endeavour is sustained by a widespread public understanding and resolve. Without this, the planners may plan and the administrators may administer, but the face of the map will nol be changed. And it wants a lot of changing. It is because your Association speaks for, and to, the public under- standing and resolve, and it is your work to do this here and throughout the country as in this your Annual Conference, that I confide to you my purposes and call on you to help me. |





